|
» Back to Table of Contents
Key Points
- This ongoing study (IIR 15-117) seeks to test the effcacy of a telephone and online problem-solving intervention in Spanish for caregivers of Veterans post-stroke.
- This study is the frst known randomized controlled trial to test a Spanish-language telephone and online intervention for caregivers in VA and addresses the need for culturally appropriate health information for an understudied population.
- The long-term goal is to partner with leaders to implement a culturally relevant, accessible, and cost-effective intervention for caregivers of Veterans post-stroke throughout VA.
Stroke is one of the leading causes of death and long-term disability in the United States. Hispanics have a higher risk of stroke-related death compared to non-Hispanics.1 Projections for 2030 indicate a 21 percent increase in prevalence of stroke among Hispanics compared to 2012.1 Those who survive a stroke often rely on informal caregivers for care and support, thus family caregivers play an important role during the stroke recovery process. Due to the abrupt nature of strokes, many caregivers experience unexpected changes and demands that they are unprepared to assume. Hispanic caregivers report higher rates of negative caregiver outcomes.2
Caregiver education and support have been recognized as important factors that help facilitate the transition home for individuals following a stroke. Providing caregivers with information, support, and skills has the potential to reduce negative caregiver outcomes and increase the likelihood that stroke survivors can remain at home.
Recognizing the important role that socio-cultural factors play in enhancing the skills of caregivers of stroke patients, and to fulfll a need for culturally relevant caregiver programs, we adapted an intervention and used a previously developed and tested Spanish-language web site: Resources and Education for Stroke Caregivers’ Understanding and Empowerment (RESCUE). This intervention has the potential to reduce caregiver depressive symptoms and burden by teaching them a creative and optimistic approach to solving caregiving related problems. To ensure cultural relevancy, we employed a rigorous cultural adaptation consisting of a dynamic and reiterative process with stakeholders. We used several sources to inform the adaptation of the RESCUE en Español intervention, including reaching a consensus among an interdisciplinary team of experts in stroke caregiving and Hispanic Veterans and families. To guide our efforts, we included input from Hispanics throughout the duration of the project, including an advisory panel. We incorporated culturally specifc graphics using low-literate and appropriate language, and verifed the translations by Spanish-speaking experts.
The study tests a telephone problem-solving intervention that uses modules, factsheets, and tools available on our RESCUE Stroke Caregiver website, Programa “RESCUE en Español.” The intervention is based on the relational/problem-solving model of stress and integrates concepts of stress appraisal and coping theory, and is based on the COPE (Creativity, Optimism, Planning, and Expert Information) framework. All study procedures and supporting materials are in Spanish.
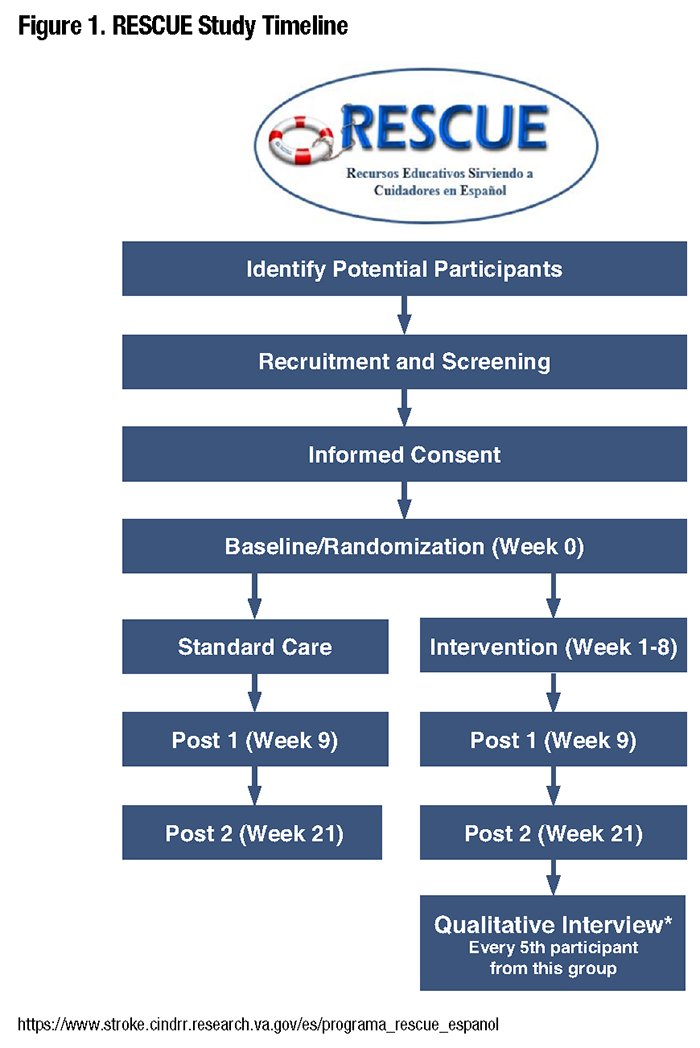
This two-arm parallel randomized controlled trial with repeated measures and mixed methods tests the effect of a telephone/ online problem-solving intervention for Spanish-speaking stroke caregivers and examines caregivers’ perceptions of the value, facilitators, and barriers to participating in the intervention. The primary outcome measure is caregiver depression. Secondary outcome measures are caregivers’ burden, self- effcacy, problem-solving, and health-related quality of life and Veterans’ functional abilities. Outcome measures are conducted at baseline and one and 12-weeks post-intervention. A budgetary impact will be conducted at the end of the study. Target enrollment is 227 stroke caregivers from three VA medical centers: San Juan, Puerto Rico, and Orlando and Tampa, Florida. Eligible caregivers who agree to participate in the study complete baseline measures and then are randomized into two groups. Participants in the intervention arm receive a nurse-led eight-session telephone problem-solving intervention and online education. Participants in the standard care arm receive normally provided VA care.
All caregivers of Veterans with a primary diagnosis of stroke who have received services from the VA Caribbean Healthcare System, Orlando VA Medical Center, or the James A. Haley Veterans’ Hospital are eligible for participation if they meet the following criteria: 1) are the self-identifed primary caregiver and provide the majority of care for a Veteran who received a diagnosis of stroke (ICD 10 codes I60.0-I69.998) within the last year and who has at least two activity of daily living defcits; 2) have Internet access and ability; 3) are reachable by cell or home phone; 4) indicate Spanish is their preferred language; 5) have moderate to severe stress; 6) self-identify as Hispanic; and 7) agree to random assignment to the intervention or standard care group. We exclude caregivers whose Veterans have a life expectancy of less than six months or are enrolled in home-based primary care or a telehealth program.
To date, we have enrolled 192 participants with 120 completed and 51 withdrawn participants. Reasons for withdrawal include Veteran’s death or placement into a residential facility, or inability to contact the caregiver. Five project modifcations have been implemented to address challenges associated with natural disasters and the COVID pandemic, including the addition of two new recruitment sites (Orlando and Tampa, Florida) and extending the duration of the project to make up for recruitment and enrollment shortages. Data analysis will begin in April 2024.
If effective, the intervention has the potential to reduce stroke caregiver depression, improve recovery of Veterans post-stroke, enable Veterans to remain in their homes, and reduce healthcare costs. This study will help identify novel interventions that can be implemented to reduce disparities for caregivers of Veterans with stroke that are sustainable in routine clinical practice and improve access to high-quality health care for minority Veterans.
- Virani SS, Alonso A, Aparicio HJ, et on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics – 2021 Update: A Report from the American Heart Association 2021 Feb 23; 143(8):e254-e743.
- Haley WE, Roth DL, Hovater M, et “Long-term Impact of Stroke on Family Caregiver Well-being: A Population-based Case-control Study,” Neurology 2015; 84(13):1323-9.
|


