|
» Back to Table of Contents
Key Points
- Facilitating the use of video telehealth is one approach to overcoming barriers that Veterans experience in accessing VA clinical and social services.
- VA distributed nearly 76,000 video-enabled tablets during the first year of the COVID-19 pandemic.
- Due to the rapid expansion of video-based care during the pandemic, QUERI investigators were able to examine how patterns of virtual care use changed across patients and VA facilities.
Access to healthcare is an overarching priority for VA as many Veterans experience barriers to VA clinical and social service use, including geographic and transportation difficulties, physical and mental health challenges, and socioeconomic stressors. Facilitating the use of video telehealth is one way to overcome these access barriers. In 2016, VA’s Offices of Rural Health (ORH) and Connected Care (OCC) began distributing video-enabled tablets to Veterans with access barriers. The Tablet Evaluation QUERI is evaluating this program to identify opportunities to improve VA tablet distribution and impact, and to examine the economic costs and benefits associated with the shift to increased video-based care.
The Tablet Evaluation QUERI is guided by the RE-AIM Framework and aims to:
- Evaluate opportunities to enhance the Reach, Adoption, and Implementation of tablets to better target high-need patients;
- Evaluate the Effectiveness of tablets on patient access, clinical outcomes, and experience, and the implementation of the VA digital divide consult;
- Examine the tablet initiative’s Maintenance potential through a budget impact analysis; and
- Evaluate shifting patterns of video-based encounters over the course of the COVID- 19 pandemic, with a focus on Veterans with high levels of clinical and social service
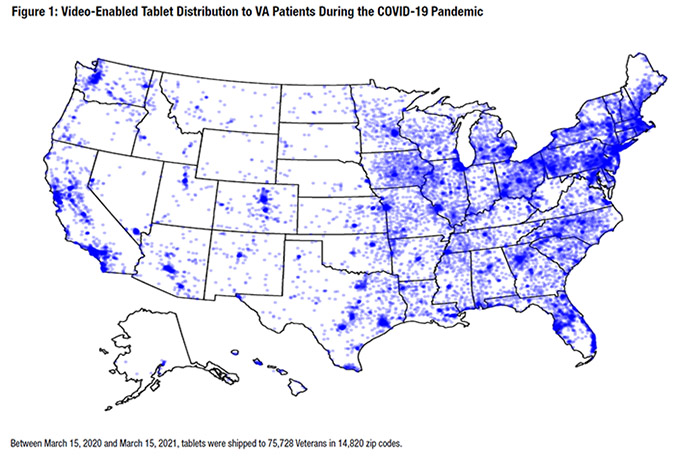
Since March 2020, video-based care has rapidly expanded as a result of the COVID-19 pandemic. VA encouraged the use of video-to-home visits because of the perceived opportunity for a more comprehensive clinical experience relative to telephone visits, as well as early evidence indicating patients’ preferences for video-based care. The tablet program has facilitated this expansion for Veterans who may otherwise not have had access to video-based care during the pandemic. Between March 1 and April 30, 2020, VA distributed tablets to more than 850 inpatient settings and more than 7,000 high-risk Veterans with access needs, a 33 percent increase from pre-COVID distribution.1 Over the first year of the COVID-19 pandemic, 75,845 patients received tablets (Figure 1). As was the case prior to the pandemic, the majority of tablet recipients (>70 percent) have a mental health condition, and tablets are most commonly used for mental health visits; however, a growing proportion of video-based visits are taking place in primary and specialty care.
Due to the rapid expansion of video-based care during the COVID-19 pandemic, Tablet Evaluation QUERI investigators examined how patterns of virtual care use varied across patients and VA facilities. Jacqueline Ferguson, PhD, evaluated the shift from in-person to video-based care early in the pandemic period and identified patient populations with lower rates of video-based encounters. 2 She found that older Veterans aged 45-64 and 65+ were substantially less likely to use video-based care compared to Veterans aged 18-44 years. Highly rural and rural dwelling Veterans were 17 percent and 12 percent, respectively, less likely to use video-based care during the pandemic compared to urban Veterans. Homeless Veterans (vs. non-homeless Veterans) were 11 percent less likely to use video care. There were minor, and likely not clinically significant, differences in video-based care by race or ethnicity. Importantly, patients with VA identified disabilities (vs. none) and patients with more chronic conditions were more likely to receive video-based care during the pandemic.
Josephine Jacobs, PhD, examined VA medical center (VAMC) video-based care uptake prior to and early in the pandemic period, assessing environmental and VAMC level factors that predict being in the top quartile of uptake.3 She found that facilities with more high-risk patients, fewer long-distance patients, and better broadband coverage had higher video- based care uptake for primary care during COVID-19. Facilities with fewer high-risk patients, fewer long-distance patients, and higher levels of video-based care use pre- COVID had higher video-based care uptake for mental health care during COVID-19.
QUERI activities are ongoing, and future work will include a patient survey and cost evaluation. In addition, to better understand the experiences of VA clinicians who are providing video-based care, our team is interviewing providers in primary care, spinal cord injury, palliative care, and cardiology. Based on interviews conducted so far, providers, though experiencing some challenges adjusting to the new technology, have mostly embraced video-based visits, finding them comparable to in-person care. Benefits of video-based visits include enhanced awareness of patients’ home environments, increased patient satisfaction, particularly for those typically travelling long distances, and more efficient use of patient-provider time. Many expressed interest in continuing to offer video-based care even after the pandemic. Providers also described several challenges that will warrant interventions in the future, including technological barriers, and the need for tools to collect vital status information and record other physical patient characteristics by video. The COVID-19 pandemic has highlighted the importance of access to telehealth and the evolving role that video-based care plays in improving access to care for Veterans. The Tablet Evaluation QUERI aims to monitor and assess the impact of video care on utilization, costs, and patient and provider experiences, to support VA and OCC’s mission to expand access to telehealth through health informatics and telehealth technologies.
- Heyworth L, Kirsh S, Zulman D, Ferguson J. "Expanding Access through Virtual Care: The VA's Early Experience with COVID-19," NEJM Catalyst July 1, 2020.
- Ferguson JM, et al. "Virtual Care Expansion in the Veterans Health Administration during the COVID-19 Pandemic: Clinical Services and Patient Characteristics Associated with Utilization," Journal American Medical Informatics Association 2021; 28(3):453-62.
- Jacobs J, et al. "Organizational and External Factors Associated with Video Telehealth Use in the Veterans Health Administration Before and During the COVID-19 Pandemic," Telemedicine and e-Health 2021.
|


