|
» Back to Table of Contents
Key Findings
- In March and April 2020, admissions to VA hospitals fell by 42 percent – likely due to pandemic-related disruptions in care.
- Admissions for appendicitis, which can sometimes be managed by antibiotics vs surgery, fell by 57 percent during this same period, suggesting that foregone healthcare may have saved some patients from avoidable procedures.
- The Disrupted Care National Project is exploring both the positive and negative effects of disrupted care during the pandemic; this work will help VA prepare for future such disruptions.
The effect on health outcomes of pandemic-related disruptions in care will be a defining public health question for our generation. Changes in healthcare utilization, particularly in the early phases of the pandemic, were profound. In March and April of 2020, admissions to VA hospitals decreased 42 percent1 and outpatient visits, either in person or remote, decreased 30 percent.2 While it is possible the 40 percent fall in admissions for events such as myocardial infarction occurred partially because people were less active, it is likely that many delayed or did not seek care at all, which could have resulted in harm to patients. Interestingly, admissions for appendicitis, a disease whose incidence would not be expected to vary because of behavior change but has been shown to be manageable in some cases with antibiotics rather than surgery,3, 4 decreased by 57 percent.1 This finding suggests that some of the foregone healthcare of the pandemic may have saved patients from avoidable interventions. The natural experiment of the pandemic is an opportunity to reveal the effects, both positive and negative, of the resulting variations in healthcare. The Disrupted Care National Project (DCNP) will explore these effects and identify areas we should focus on during the pandemic recovery. As we move forward, we will further develop the conceptual framework depicted in Figure 1 by adding more potential confounders or pathways as they come to light.
The DCNP has both research and coordinating center components. It is led by Contact Principal Investigator (PI) Louise Davies at White River Junction Medical Center (WRJ), with WRJ also serving as the Coordinating Center for the HSR&D disrupted care agenda. Multiple PIs Amy Justice at West Haven, and Anita Vashi at Palo Alto, bring deep expertise to the research and coordinating center work for the DCNP. The overall goal of the DCNP is to characterize how the COVID-19 pandemic affected healthcare delivery and outcomes for Veterans to create a research roadmap for future work in this area. The analyses will inform priority setting during the recovery from the pandemic and preparations for future disruptions.
To begin, the DCNP is performing parallel ecologic analyses of VA data, U.S. population data from the Centers for Disease Control and Prevention (CDC), and Medicare population data from the Centers for Medicare and Medicaid Services (CMS). These analyses will place the VA experience in context, by comparing excess mortality overall, within demographic and diagnostic subgroups, and by calendar month. The analyses will test for associations between mortality trends and changes in healthcare utilization.
We will then take full advantage of the richer, patient-level electronic health record data available within VA to better understand how much of the excess mortality is likely attributable to COVID-19 by using a risk index for undiagnosed cases and examining how it is distributed across specific demographic and diagnostic subgroups. Last, the DCNP will examine the effects of disruption in care on Veteran outcomes for chronic illnesses such as hypertension and surgical procedures.
Coordinating Center activities are designed to accelerate progress, ensure sharing of knowledge, and to consider the needs of stakeholders. The Coordinating Center will also work to reduce duplication of efforts by supporting a community of closely collaborating investigators in the disrupted care space. Specific activities currently underway include the following.
- Regular convening of a Steering Committee made up of operational partners within VA and planned communications with external stakeholders who share an interest in the findings.
- Creation of forums to facilitate the curation of data and research methodologies.
- Establishment of research definitions related to disruptions in care.
- Development of a platform(s) for in-depth research discussions regarding research methods, ideas, and definitions, and sharing of static reference materials related to the pandemic.
The DCNP will characterize how the COVID-19 pandemic affected healthcare delivery and outcomes for Veterans, inform priority setting during the recovery from the pandemic, and help with preparations for future disruptions. Through coordination with all investigators working in this area, the science will advance efficiently, and findings will be shared broadly with partners and stakeholders.
Below are links to other HSR&D funded projects in the disrupted care space.
Figure 1. Conceptual Framework of the Impact of Disruption in Care on Changes in Mortality
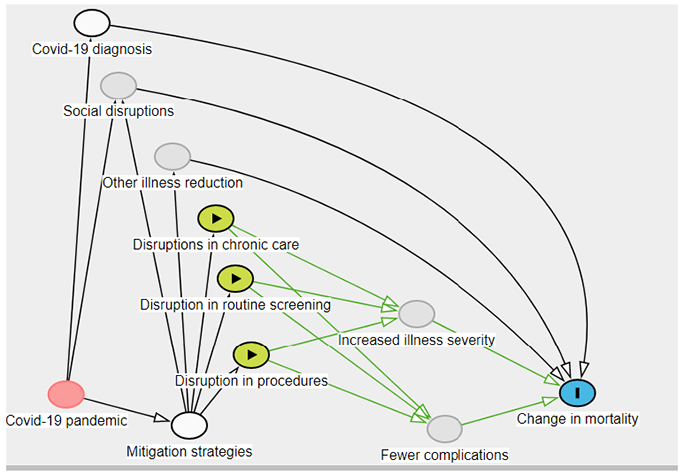
Mitigation strategies include lockdown and social distancing, imposed by both government and individual choice; COVID-19 diagnosis includes diagnostic codes and PCR/antigen tests; social disruptions include economic loss or substance use; other illness includes reductions in influenza; change in mortality represents both excess mortality and reductions in population-level mortality.
- Baum A, Schwartz MD. “Admissions to Veterans Affairs Hospitals for Emergency Conditions During the COVID-19 Pandemic,” JAMA 2020; 324(1):96-9.
- Baum A, Kaboli PJ, Schwartz MD. “Reduced In-Person and Increased Telehealth Outpatient Visits During the COVID-19 Pandemic,” Annals of Internal Medicine 2021; 174(1):129-31.
- Park HC, Kim MJ, Lee BH. “Randomized Clinical Trial of Antibiotic Therapy for Uncomplicated Appendicitis,” The British Journal of Surgery 2017; 104(13):1785-90.
- Collaborative C, Flum DR, Davidson GH, et al. “A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis,” New England Journal of Medicine 2020; 383(20):1907-19.
|


